About the LittleEARS website
You have been invited to use this website as the GP or audiologist has diagnosed your child with glue ear. This website will give you information about the condition, treatments that are available and some guidance about how to help your child.
Please use the menu or the page links at the bottom of each page to find out the information you need.
You may know some things already but it is a good idea to look through all of the site as there may be some new useful information.
You don't have to look at everything today.
You can log out and come back whenever you like.
About glue ear
Glue ear (medical term: otitis media with effusion) is a condition where there is a build-up of fluid in the middle ear (the part of the ear just behind the eardrum).
The middle ear is normally filled with air which allows the eardrum and small ear bones to vibrate in response to sound. In glue ear, the middle ear fills with fluid which reduces the sound vibrations and hearing can be affected.
Dr Ian Williamson, GP and researcher at University of Southampton talks about the causes of glue ear and the effect it can have on children (2 mins)
To move on through the website, please use the links below. Next section: What causes glue ear?
What causes glue ear?
The build-up of sticky fluid in the middle ear can be caused by a problem with a part of the body called the Eustachian tube.
The Eustachian tube is a thin channel which connects the middle ear with the back of the nose. Most of the time this tube is closed, but when you swallow or yawn, the tube opens to let the air in and any fluid drain out..
Diagram of the ear:

In children with glue ear:
The Eustachian tube can become blocked with mucus, often after a recent cold or ear infection. This stops air entering the middle ear and fluid draining out.
Young children have narrow and horizontal Eustachian tubes which means they can often get blocked.
As children get older, the Eustachain tubes become wider and more upright which allows fluid to drain better. This is why children often grow out of glue ear.
What are the symptoms?
Most common symptoms:
Hearing loss: When children have glue ear their hearing levels can be similar to wearing ear plugs or putting fingers in their ears.
Common symptoms of glue ear include:
- Often mishearing what is said, especially in noisy environments
- Needing the television volume turned up
- Saying ‘eh what’ or ‘pardon’ a lot
- Appearing to lip-read.
Physical ill health: children with glue ear can show symptoms of physical ill-health such as:
- Repeated ear infections (glue ear often follows acute ear infections, colds and flu)
- Snoring, blocked nose or poor sleep
- Noises in the ear or dizziness
- Clumsiness or off-balance.
Long term or persistent glue ear:
If glue ear has been present for a long while you may notice some of the following symptoms:
- Children with glue ear can become frustrated, feel left out and become quiet and withdrawn.
- You may notice that your child is not doing so well at school as expected.
- Your child’s speech and language may appear to be behind other children of similar age.
These symptoms are less common as glue ear normally gets better in 3 months without any treatment. However, if you are particularly concerned about your child's behaviour, educational or speech/language development you can contact your child's GP or health care provider at any time.

How common is glue ear?
Glue ear is extremely common, especially in children aged between 1 and 6 years, although it can develop at any age.
- One in five children will be affected by glue ear in the first year of primary school and 80% of children will have at least one episode by the age of 10 years old.
Children can have glue ear in one or both ears.
- 40% of children with glue ear will have it in both ears.
Glue ear is just as common in boys as in girls.
It is more common in the winter months when there are lots of coughs and colds.

Can glue ear be prevented?
Doctors aren't exactly sure what causes glue ear so there is no way to prevent it in the majority of cases.
However, children often develop glue ear after a cold or an ear infection so there are a number of steps you can take to try and reduce the risk of children getting glue ear:
- Smoke-free environment: Children who live in a smokey environment are more likely to get ear infections and glue ear. Try to make sure that your child's environment is kept smoke-free.
- Childhood vaccinations: It is likely that childhood vaccines will reduce the number of ear infections that children get. Keeping your child's vaccinations up to date may help to prevent glue ear (click here for childhood vaccination schedule).
- Frequent handwashing can be helpful to prevent the spread of viral infections in families. Remind your child to wash their hands regularly, especially before eating and after school.

How is glue ear diagnosed?
Medical history
Your child's medical history helps the doctor, nurse or audiologist (hearing specialist) to diagnose glue ear. In particular they are interested in certain symptoms which can indicate hearing problems:
- Recent research found that children who mishear, turn the TV volume up loud and report any ear-related problem in the previous 3 months are more likely to have glue ear.
Common tests for glue ear include:
Otoscopy is a procedure where your child’s doctor, nurse or audiologist looks into your child’s ear using a medical device called an otoscope to see the ear canal and eardrum. In children with glue ear, the eardrum can look cloudy, be pulled back into the middle ear and sometimes bubbles and fluid can be seen behind the eardrum.

Tympanometry is a simple test for fluid in the middle ear. The tympanometer measures the movement of the eardrum to a change in air pressure. The eardrum moves freely when the pressure inside and outside the ear is the same. When there is fluid in the middle ear, the eardrum does not move so well and sound waves bounce back rather than pass through to the middle ear. The test only takes a few seconds and doesn't cause any discomfort.
Audiometry is a test of hearing levels and is normally carried out by an audiologist (hearing specialist). There are different tests depending on the age of your child.
- Play audiometry is designed for children between 2-5 years and uses games, such as placing a block in a basket or ring on a cone, when they hear a sound. This makes testing fun and engaging for children. Children will wear headphones and the audiologist will test their hearing over a range of sounds and frequencies.
- Visual reinforcement audiometry is a test for very young children who are too young for play audiometry (designed for children aged 6 months to 2-3 years). The test uses visual reinforcement such as video animations or lighted toys placed to each side of the child and children are trained to look at the stimulus when they hear a sound. Children will often sit on a parent’s/carer’s lap and may wear lightweight earphones whilst taking the test.
- Pure-tone audiometry is a test for older children and adults. A range of sounds are played through headphones and patients respond by pressing a button.

Helping your child with glue ear
If your child has been diagnosed with glue ear, your doctor, nurse or audiologist will recommend watchful waiting to see if your child’s glue ear clears up on its own. Watchful waiting is a period of time in which a medical problem is monitored to see if it gets better on its own, stays the same or gets worse.
- 50% of children get better with watchful waiting in 3 months and 90% will have normal hearing at 1 year.
How to help during watchful waiting
- Helping your child to hear better: helping your child to listen and concentrate at home and school can help with their behaviour and reduce frustration for both you and your child (see next section for advice).
- Monitoring progress: keep a close eye on your child's hearing symptoms to check for improvements or need for further advice. You can download here a symptom diary to help you monitor your child's symptoms.
- Recognising when you need more help: if you think that your child's symptoms are getting worse or lasting longer than 3 months you may need to get more advice from the school nurse or your child's GP/nurse.

Helping at home

Whilst waiting for your child's glue ear to clear up, there are lots of things you can do to help your child listen and concentrate. This can help with their behaviour and reduce frustration for both you and your child.
- Reducing background noise: Turn off the TV or radio if you are playing with or talking to your child. Background noise can make it difficult for your child to hear conversations.
- Get their attention: Before speaking to your child or giving them instructions, make sure you get their attention first. This lets them know that you are trying to talk to them.
- Face them when talking: Ensure that your child can see your face when talking to them so they can use lipreading cues to help them understand what you are saying.
- Make lipreading easy: Lip-reading is a technique of understanding speech by carefully watching movements of the face, lips and tongue, when sound levels are low or missing. Whilst mostly used by people with reduced hearing, people with normal hearing also lipread subconsciously (children as young as 19 months old have been shown to lip-read). Speak clearly and naturally at a normal pace to help your child to use lipreading cues.
- Give brief, clear instructions: Use short instructions rather than long sentences. This will make sure that your child understands the main points.
- Check your child's response to make sure that they have understood you correctly
- Speak to your child's teacher: let your child's teacher know about their glue ear so they can take appropriate action in the classroom.
Helping at school

If you let your child's teacher know that they have glue ear, the teacher can help them in the classroom. The following is a list of the things that teachers may be able to do to help your child:
-
Reducing background noise in the classroom, especially when giving instructions
-
Ensuring your child is sitting where they can see the teacher.
-
Gaining your child’s attention before giving instructions
-
Using short, concise sentences for instructions.
-
Writing key words and instructions on the board
-
Speaking clearly, at normal speed.
You can download some information for your child's teacher to help them to understand the hearing difficulties your child has and how they can help them in the classroom (download information for teachers here)
Nasal balloon treatment
Your child's doctor, nurse or audiologist may prescribe treatment with a nasal balloon to help clear your child's glue ear during the watchful waiting period.
Treatment involves your child blowing up a medical balloon with their nose 3 times a day for 1 to 3 months or until the fluid has cleared and their hearing has returned to normal.
The treatment is suitable for children from about the age of 4 years old, although children as young as 3 have been reported as able to inflate the nasal balloon.

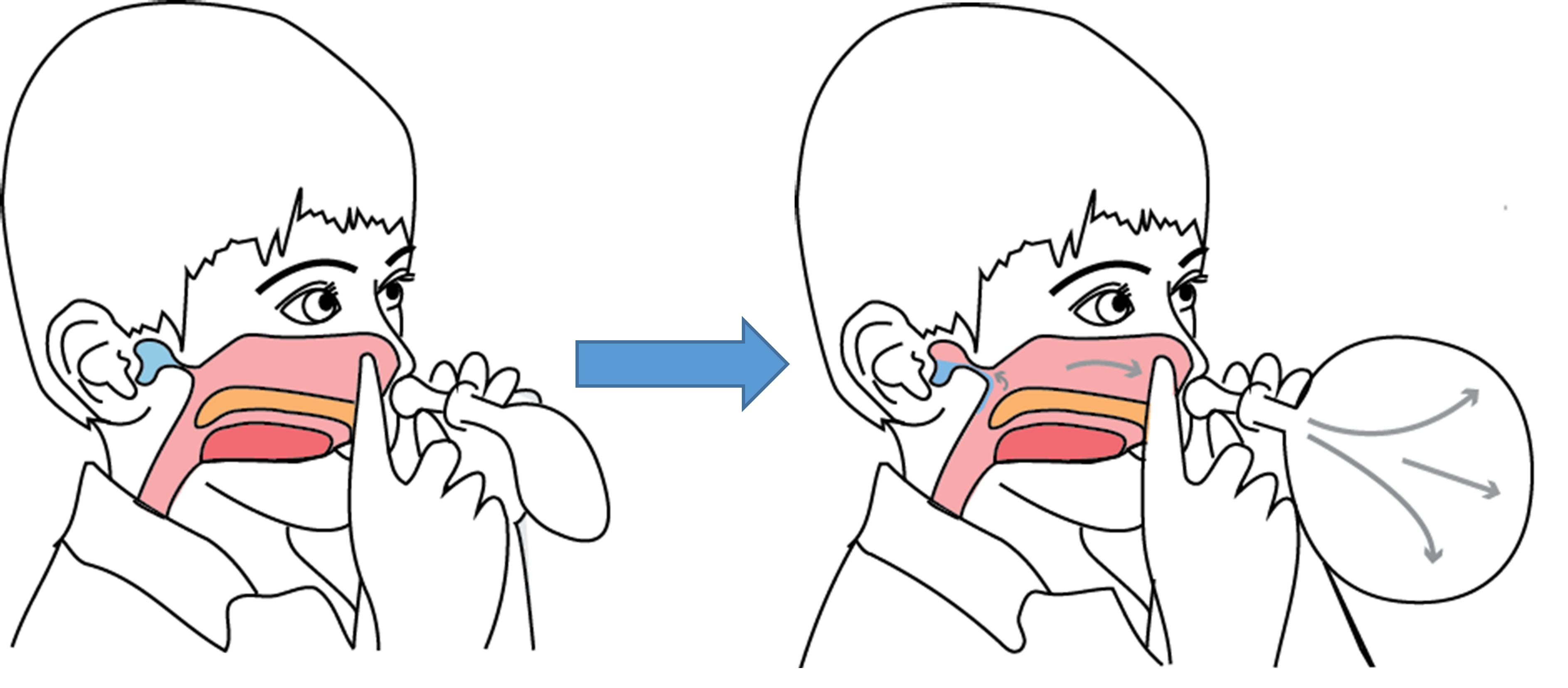
How does it work?
The pressure of blowing a balloon up with the nose opens the Eustachian tubes. This lets air in to the middle ear and allows fluid to drain out. Regular nasal balloon treatment can help your child's hearing to return to normal.
What is the evidence?
- Recent research has found that children who use the nasal balloon were 40% more likely to have their ears cleared of fluid after 1 month compared to children who had watchful waiting alone.
- Children who use the nasal balloon also had fewer days with symptoms and better quality of life than children who had watchful waiting after 3 months.
How often do they need to inflate the balloon?
The balloon needs to be inflated 3 times per day in each nostril, for example in the morning, after school and before bed. It is good to try and make blowing up the balloon part of your child's daily routine like when they are cleaning their teeth.
Are there any side effects?
Your child might notice a popping or clicking sound when they blow up the nasal balloon, especially the first time. These effects are normal and can indicate that the Eustachian tubes are opening and the treatment is working. (The effect is similar to equalising pressure in your ears when on an aeroplane).
Runny noses have been reported in a small number of children using the nasal balloon.
When should my child NOT use the nasal balloon?
Ear infection: The nasal balloon should not be used if your child has an ear infection.
Cold or blocked nose: if your child develops a cold or blocked nose it is best to stop the balloon for a few days until their airways clear, and then start up again.
Nasal balloon instructions
The nasal balloon comes in a treatment pack (Otovent) containing 5 medical balloons, a connecting nozzle and a small carrying case.
Watch a video demonstration of nasal balloon autoinflation here (1min 26secs):
Step by step instructions:
- Take one of the balloons and stretch it using your hands or blow it up with your mouth to release some of the tension, otherwise the first inflation may be quite difficult.
- Attach the balloon to the connecting nozzle.

- To make sure your child understands what they need to do either show them the instruction video or demonstrate the nasal balloon yourself.
- Ask your child to hold the nozzle up to one nostril and close off the other nostril with their fingers.
- Instruct your child to keep their mouth closed, slowly blow out of the nose and inflate the balloon to about the size of a large orange. Repeat with the other nostril.
- Give lots of feedback and encouragement. Using a sticker chart can help you and your child to remember to use the balloon regularly (download sticker chart here)
What do parents say?

Parents of children who took part in a research study at University of Southampton were interviewed about the nasal balloon. Here are some of their experiences:
What did parents say about the nasal balloon?
Most parents and children liked the idea of trying a nasal balloon to treat glue ear and children found it fun to do:
- One mother of a 5 year old boy said "it looked quite a simple thing to use and – he just got on with it. He loved it, you know, it was a great thing, a five-year-old boy trying to blow up a balloon with his nose"
- Another parent agreed: " well the girls thought that was great fun, anything to do with balloons!"
What helped them remember to use the nasal balloon?
Parents said that making the nasal balloon treatment part of their daily routine was helpful. The children liked using a sticker reward chart as a reminder (you can download a sticker reward chart here)
- Parent of 6 year old boy commented: "in the morning whatever we were doing, and then at bedtime, so it was just like cleaning your teeth, just brought it in as an extra thing to do as part of the routine”
- Parent of 4 year old boy commented: “he was – really happy to be down here: let me mark off, let me put the sticker on – and so we never had no problems with it. In fact he was reminding me – mum, I haven't done it, I haven't done my balloon”
Did families have any problems using the nasal balloon?
Some parents reported that their children had problems with the first inflation. Pre-stretching really helps with releasing some of the tension and to keep trying.
-
Parents of a 6 year old boy said: "He did struggle to start with, but it wasn't long before he could get it to an orange"
-
Another parent agreed "my son was quite shy to do it at first. But when we got home of course it's like a new toy so he was all over it"
Other parents reported problems continuing treatment over a longer period. Parents tried to make the treatment fun for the children:
- One parent commented: "We made a joke out of it; it was a bit of a game really - to see who could blow the biggest balloon"
- Mother of a 4 year old girl said: " It got tricker as time went on because she got fed up with it and she was saying she didn't want to do it anymore. But i kept encouraging her and gave her sticker rewards and she managed to finish the treatment"
FAQ - nasal balloon treatment

Where can I get a nasal balloon?
The nasal balloon (Otovent) is available on prescription from your child's GP or can be purchased from the chemist or from the internet.
How often do they need to inflate the balloon?
The balloon needs to be inflated 3 times per day in each nostril, for example in the morning, after school and before bed. It is good to try and make blowing up the balloon part of your child's daily routine like when they are cleaning their teeth.
How do your know when to change the balloon?
The balloon should be changed every week, or when it seems to have lost tension (your child may report that it is no longer working). The nozzle can be wiped with an antiseptic/baby wipe or washed in warm soapy water.
Are there any side effects to the nasal balloon?
Your child might notice a popping or clicking sound when they blow up the nasal balloon, especially the first time. These effects are normal and can indicate that the Eustachian tubes are opening and the treatment is working.
Runny noses have been reported in a small number of children using the nasal balloon.
When should my child NOT use the nasal balloon?
The nasal balloon should not be used if your child has an ear infection or if they have a latex allergy.
If they have a cold or blocked nose, it is probably best to stop the balloon for a few days until their airways clear, and then start up again.
How can you help your child manage the nasal balloon?
Give lots of encouragement when your child blows the balloon up for the first time. Sometimes they will only manage a small inflation but this can be enough to have a treatment effect. Most children can manage it with some practice .
Other treatments
For most children, the middle ear fluid should clear up in 3 months and watchful waiting is the best management strategy.
Non-surgical treatments
Medical treatments like antibiotics, antihistamines, decongestants and nasal steroids are sometimes given to children with glue ear, but there is no evidence that they are effective and some of them have unwanted side effects.
Alternative and complementary therapies like osteopathy, chiropractic and homeopathy are not currently recommended for glue ear as there is not enough evidence that they work.
Temporary hearing aids are an option for some children with hearing difficulties associated with glue ear. They can help children distinguish between background noise, such as general classroom sounds, and foreground noise such as conversation and the teacher speaking.
- You can find more information about hearing aids from the National Deaf Children Society (NDCS website) or speak to your child's healthcare provider.
Surgical treatments
If your child has long term problems with hearing loss in both ears, and there are concerns that your child has behavioural /educational problems or speech and language delay they may be referred to an ear, nose and throat (ENT) specialist to discuss surgical options (grommet surgery).

Operations for glue ear
Grommet surgery
Grommet surgery involves a small operation under general anaesthetic where fluid is drained from the middle ear and a ventilation tube (grommet) is inserted in the eardrum to allow air into the middle ear.
Removing the fluid from the middle ear helps the sound vibrations transfer to the inner ear to improve hearing, and the grommet keeps the air flowing into the middle ear to stop the glue ear returning.
Who is grommet surgery suitable for?
Grommet surgery is an important treatment for a small minority of children with long term glue ear in both ears, and with speech, language and educational development problems.
- Watchful waiting is the best management strategy as middle ear fluid will clear up on its own in 90% of children in 12 months.
How effective is grommet surgery?
Grommet surgery is an effective, short-term treatment for glue ear. Hearing levels are improved for the first 6-9 months after the operation, but by 12-18 months there is no difference between those children who did and did not have surgery (children who don't have surgery get better on their own).
- Grommet surgery does not cure the underlying cause of glue ear. Instead it improves hearing to allow for normal learning and development whilst children grow out of glue ear.
What are the problems associated with grommet surgery?
Having grommet surgery means that your child will need to have a general anaethetic. Often children will have ear discharge after surgery, and there is a small risk of scarring or permanant perforation of the eardrum.
Grommets normally fall out of the eardrum after 6-12 months and in up to 50% of cases another operation is needed within 5 years.
Adenoid surgery
Adenoids are small clumps of glandular material at the back of your nose and are part of your immune system used to fight infection. Sometimes the adenoids become swollen and can block the opening of the Eustachian tubes. Removing them can help the Eustachian tubes work better and help with glue ear. Normally adenoids are taken out at the same time as grommet surgery, or when tonsils are removed.
What to do next
Monitoring your child's hearing
It is recommended that you monitor your child over a period of 3 months to check for improvements in their hearing. You can use the LittleEARS hearing disability test to check if your child is at risk of hearing problems.
Hearing has improved?
If your child appears to be hearing satisfactorily there is no need to do anything further.
Keep monitoring: Glue ear can come and go, especially in the winter months, so you may want to keep monitoring during this period. You can also take the LittleEARS hearing test again with your child if you have concerns in the future.
If symptoms return: Your child can use the nasal balloon again if their symptoms return.
Still concerned?
If you are still concerned that your child is not hearing you, has ongoing speech or language problems or is not doing as well at school as you/your child's teacher thinks, we suggest that you make a further appointment with your child's GP for advice.

Quick links
You will find here quick links to some of the important links and downloads from the website:
The LittleEARS hearing disability test
Links to videos
Links to print sheets
Other useful information
Meet the researchers
